Infectious Disease
Common Bacterial Infections
Common Viral Infections
Common Fungal Infections
Common Parasitic Infections
Malaria
Ascaris lumbricoides
Enterobius vermicularis
Hookworm
Strongiloides stercoralis
Trichuris trichiura
Enterobius vermicularis
Capillaria
Trichinella
Gnathostomiasis
Angiostrogylosis
Wuchereria bancrofti
Opisthorchiasis
Paragonimus westermani
Schistosomiasis
Diphyllobothrium latum
Taeniasis
Neurocysticercosis
Scabies
Head/Body/Pubic Lice
Ascaris lumbricoides
Enterobius vermicularis
Hookworm
Strongiloides stercoralis
Trichuris trichiura
Enterobius vermicularis
Capillaria
Trichinella
Gnathostomiasis
Angiostrogylosis
Wuchereria bancrofti
Opisthorchiasis
Paragonimus westermani
Schistosomiasis
Diphyllobothrium latum
Taeniasis
Neurocysticercosis
Scabies
Head/Body/Pubic Lice
Systemic Approach to Infection
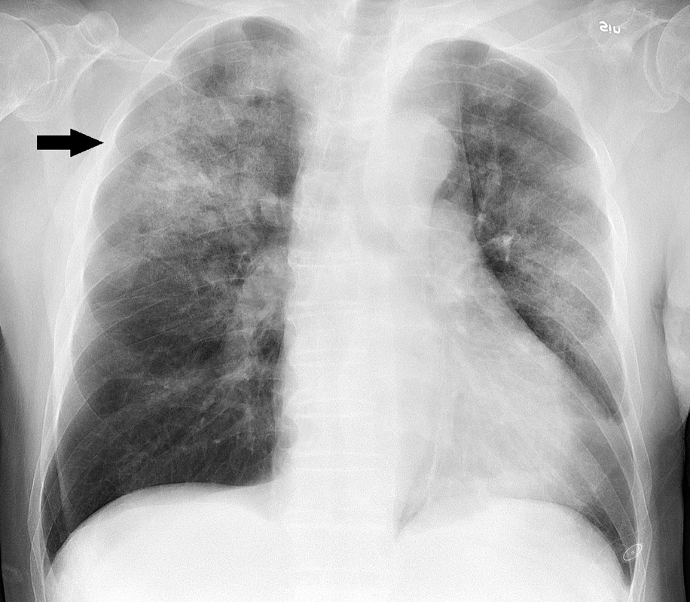
Pneumonia
- Acute lower respiratory tract infection associated with changes visible on CXR
- Classification
- Community acquired = up to 48 hours since admission, common pathogens: S. pneumoniae, H. influenza, M. catarrhalis, Atypicals (M. pneumonia, S. aureus, Legionella, Chlamydia)
- Hospital-acquired pneumonia = 48 hours or more after admission. Common pathogens: Gram negative enterobacteria, S. aureus, P. aeruginosa, Klebsiella, Bacteroides, Clostridia
- Aspiration pneumonia: associated with stroke, bulbar palsy, poor dental hygiene. Common pathogens: anaerobes
- Immunocompromised host: Pneumocystis jirovecii, mycobacteria, fungi, viruses
Signs and symptoms
- Fever, rigors, tachypnoea, tachycardia
- Purulent sputum, haemoptysis
- Pleuritic chest pain
Investigation
- Blood tests (CBC, CRP, LFT, U+E’s, haemoculture)
CURB-65 Scoring System
- C: Confusion (1)
- U: BUN ≥ 19 mg/dL (1)
- R: Respiratory Rate ≥ 30/min (1)
- B: Systolic BP ≤ 90 mmHg or Diastolic BP ≤ 60 (1)
- 65: Age ≥ 65 (1)
- Chest X-ray
- Chest ultrasound (for pleural effusion, empyema)
- Urine antigen (if suspecting Pneumococcal spp (CURB ≥ 2) or Legionella spp. (CURB ≥ 3))
- Bronchoalveolar lavage (chronic infection, ?TB, immunocompromise)
Management
- Community-acquired pneumonia (empirical)
- CURB = 0-1 → amoxicillin 500mg -1 g tid PO or clarithromycin 500 mg bid or doxycycline 200 mg loading + 100 mg od for 5 days
- CURB = 2 → amoxicillin + clarithromycin or doxycycline (same dosage as above). Alternatively IV amoxicillin 500 mg tid + clarithromycin 500 mg bid for 7 days
- CURB = 3 or more → IV co-amoxiclav 1.2 g tid OR IV cephalosporin + clarithromycin 500 mg bid for 7 days
- If Staphylococcal → flucloxacillin + rifampicin. Vancomycin if MRSA suspected.
- Atypical: Legionella → clarithromycin + fluoroquinolone, Chlamydia → tetracycline, Pneumocystis → co-trimoxazole
- Hospital-acquired pneumonia
- IV aminoglycoside + IV piperacillin-tazobactam or IV cephalosporin (3rd gen)
- Aspiration pneumonia
- IV cephalosporin + IV metronidazole
- Neutropaenic patient
- Same as hospital-acquired, may add antifungals if no improvement after 48 hours
Note:
- Streptococcus pneumoniae: most common, more common among hyposplenic/asplenic, pre-existing lung disease or immunocompromised patients
- Staphylococcus: common after influenza, in CF patients, may cause bilateral cavitating bronchopneumonia
- Klebsiella: more common among diabetics, alcoholics, elderly, can cause upper lobe cavitating bronchopneumonia
- Pseudomonas: more common among CF, bronchiectasis and hospital-acquired pneumonia patients
- Mycoplasma: causes reticular nodular or patchy consolidation → worse CXR than clinical status, associated with cold agglutination autoimmune haemolytic anaemia
- Legionella: colonized water tanks/AC, associated with lymphopaenia, hyponatraemia, deranged LFT
- Pneumocystis: more common among immunocompromised patients, bilateral perihilar interstitial shadowing
- Chlamydophila psittaci: from birds, may cause arthralgia, endocarditis, meningoencephalitis
Complications of pneumonia
- Respiratory failure
- Septic shock
- Pleural effusion, empyema or lung abscess
- Atrial fibrillation
Reference: Oxford Handbook of Clinical Medicine (10th Ed)