Chest Medicine
Obstructive Lung Disease
Restrictive Lung Disease
Pulmonary Vascular Diseases
Neoplasms of the Lungs
Pleural Disease
Other Respiratory Disorders
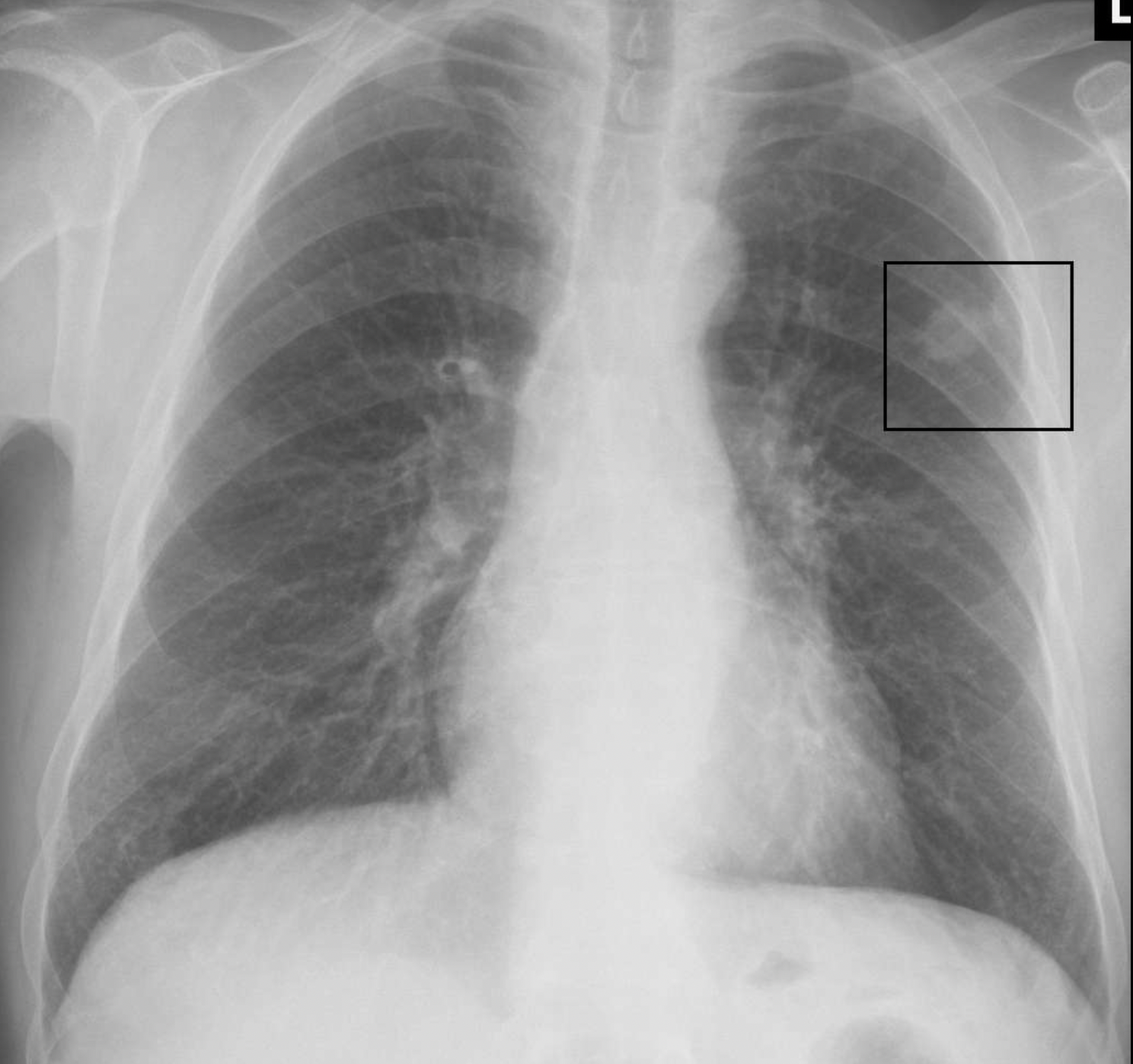
Solitary Pulmonary Nodules
- Common incidental finding on CXR
- May be entirely symptomatic or may present with cough and dyspnoea
- May be associated with smoking and second-hand smoking → increased risk of lung cancer
Investigation
- Consider CT chest as the next investigation
- If the nodule has fat or calcification characteristic of a benign lesion (hamartoma or granuloma) → no further evaluation required
- If reassuring features are absent → review previous CT if available
- If old CT available, nodule old AND no progression in size over 2 years → no further evaluation required
- If old CT not available OR progression in size OR new nodule → determine risk of malignancy
| Feature | Low Risk | Intermediate Risk | High Risk |
|---|---|---|---|
| Diameter (cm) | < 0.8 | 0.8-2 | ≥ 2 |
| Age (years) | < 45 | 45-60 | ≥ 60 |
| Smoking Status | Never | Yes | Yes |
| Years since smoking cessation (if applicable) | > 15 | 5-15 | < 5 |
| Nodule characteristics on CT | Smooth | Scalloped | Corona radiata or spiculated |
| Benign | Malignant |
|---|---|
| Age < 35 years | > 45-50 years of age |
| Non-smoker | Smoker |
| No change from old films | New or enlarging lesions |
| Central, uniform or popcorn calcification | Absent or irregular calcification |
| Smooth margins | Irregular margins (scalloped or spiculated) |
| Size < 2 cm | Size ≥ 2 cm |
Management
- Low risk: serial CT scans
- Intermediate risk: biopsy or PET
- High risk: surgical excision
Reference: First-Aid for the USMLE step 2 CK (10th Edition)