Gastrointestinal
Oesophageal Disease
Disorders of the foregut
Small Intestine Disease
Large Intestine Disease
Inflammatory Bowel Disease
Liver and Biliary Disease
Pancreatic Disease
Gall stones disease: Clinical Practice Guideline
- Clinical presentation: majority of patients are asymptomatic (approximately 15-25% will be symptomatic after 10 to 15 years of follow-up)
- Symptoms of biliary colic: intense but dull RUQ, epigastric or less frequently substernal pain, may radiate to the back. Pain is associated with fatty meals, vomiting, nausea and/or sweating. Pain often constant but can be colicky.
- Pathophysiology: neuronal or hormonal stimulation of the gallbladder → contraction → stone pushed against outlet or cystic duct → ↑ intra-gallbladder pressure → pain (Murphy's sign = Pushing/Palpating of the RUQ during inspiration leads to respiratory arrest)
Investigation
- Bloods: CBC, Bilirubin, LFT (ALT, AST, ALP), Gamma glutamyl transferase (GGT), Amylase, Lipid profiles
- Imaging: first-line ultrasound abdomen (gallstones are echogenic with shadows)
- Other modalities: abdominal X-ray → may show calcified gallstones
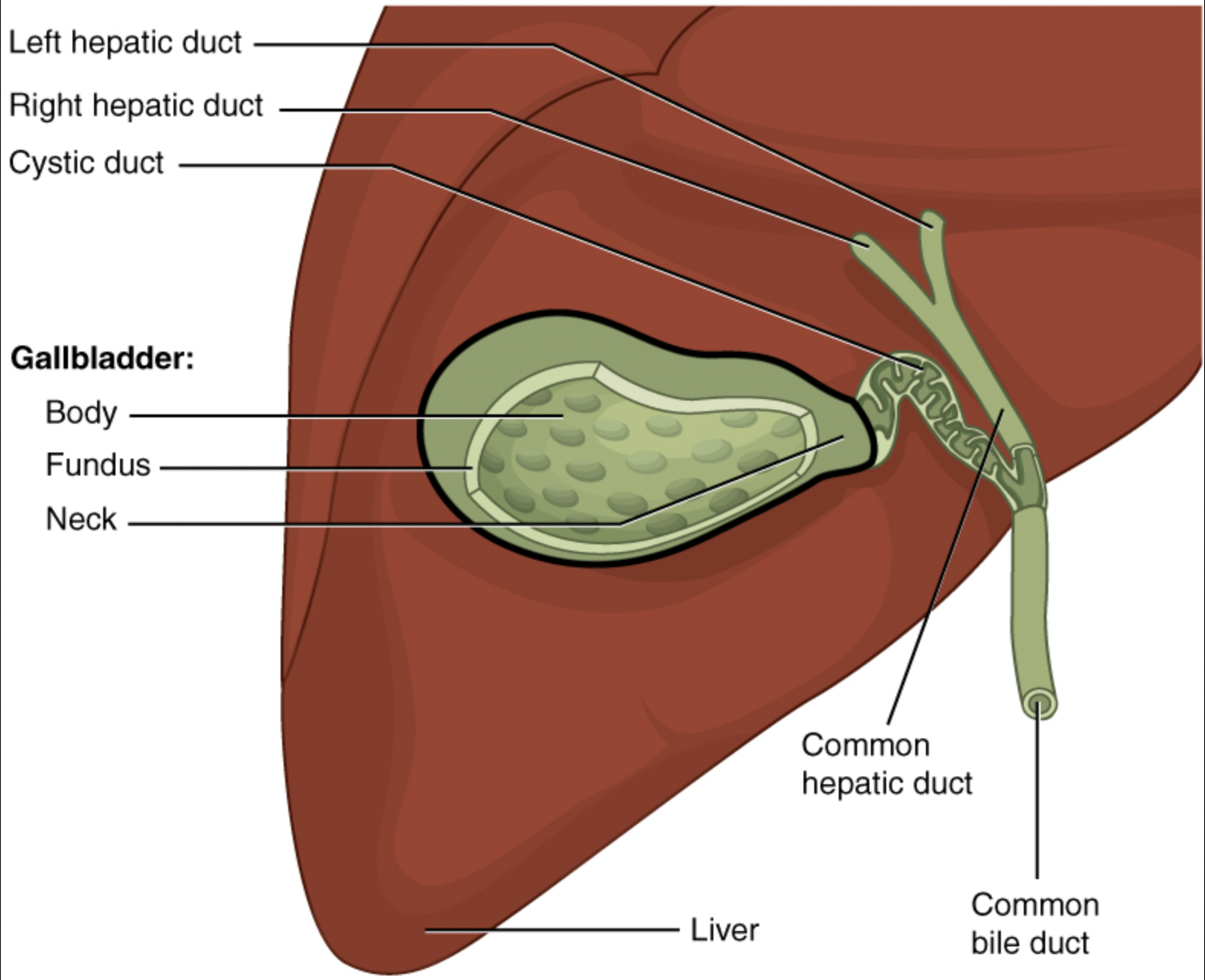
| Diagnosis | Location of obstruction | Signs + symptoms |
|---|---|---|
| Biliary colic | gallstones in the gallbladder | Colicky pain esp. with food |
| Acute cholecystitis | gallstones in the cystic duct | Constant RUQ pain |
| Ascending/acute cholangitis | gallstones in the common bile duct | RUQ pain + fever + jaundice |
Management
- Gallstones present + asymptomatic → no treatment required, advice given regarding complications and lifestyle modifications
- Gallstones present + symptomatic → advise surgery
- Biliary colic → elective laparoscopic cholecystectomy
- Acute cholecystitis
- If presents within 72 hrs → laparoscopic cholecystectomy
- If presents > 72 hrs → may consider IV antibiotic treatments until stabilise before laparoscopic cholecystectomy
- Ascending cholangitis
- Treating sepsis (IV fluids and antibiotics)
- Biliary drainage e.g. ERCP or percutaneous transhepatic cholangiography
- Management of underlying cause: elective laparoscopic cholecystectomy
- Consider open instead of laparoscopic cholecystectomy if
- Patient needs an open laparotomy for other indication(s) at the same time
- Patient has complicated pathology e.g., acute gangrenous cholecystitis, acute empyema, or liver cirrhosis
Reference:
- The Royal College of Surgeons of Thailand
- UpToDate - Gallstone Diseases