Gastrointestinal
Oesophageal Disease
Disorders of the foregut
Small Intestine Disease
Large Intestine Disease
Inflammatory Bowel Disease
Liver and Biliary Disease
Pancreatic Disease
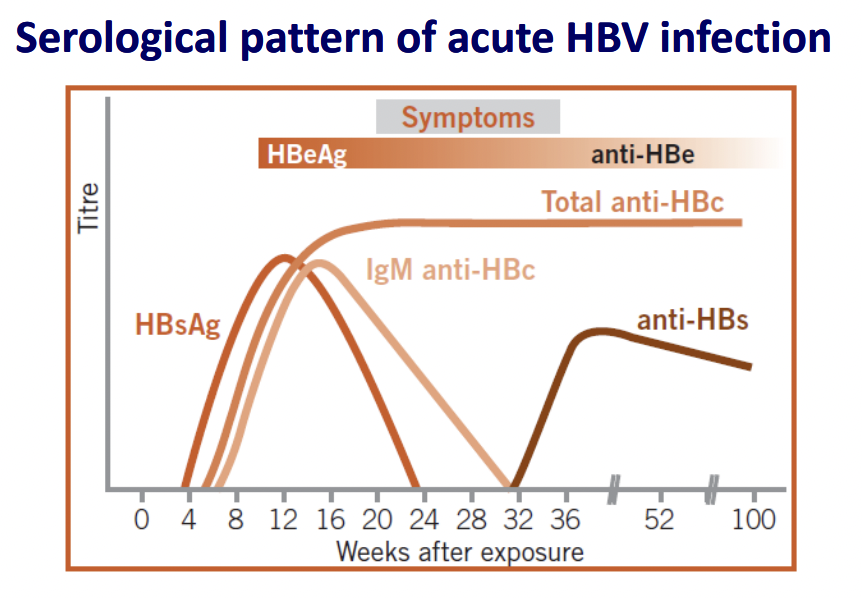
Acute viral hepatitis
Signs and symptoms
- Fatigue, malaise, fever and jaundice
- May be asymptomatic
- Signs: tender hepatomegaly
Investigation
- LFT: ALT > 10 x normal limit, AST > ALT (in the first 24-48 hours), direct hyperbilirubinaemia
- Viral hepatitis serology
- HAV: anti HAV-IgM
- HBV: HBsAg, anti-HBc-IgM
- HCV: HCV RNA
Management
- Symptoms management + supportive care
- F/U LFT in 1-2 weeks
- Dietary advice: avoid high-carb diet (may induce fatty liver disease), avoid fatty diet if abdominal pain persists
- Admit if any of the following:
- Severe symptoms: nausea/vomiting, encephalopathy
- Bilirubin > 15-20 mg/dL
- Prolonged hyperbilirubinaemia > 2 weeks
- Prolonged PT with rapidly falling AST/ALT
- Hypoglycaemia
- Hepatocellular failure (drops in albumin, ascites)
Prevention
Pre-exposure prophylaxis for HAV
| Age (years) | Vaccine | Dose |
|---|---|---|
| 1-15 | Havrix 360 | 3 (0, 1, and 6 months) |
| 16-18 | Havrix 720 | 2 (0 and 6-12 months) |
| 19 and above | Havrix 1440 | 2 (0 and 6-12 months) |
Post-exposure prophylaxis for HAV
- Indications
- Household or sexual contacts with infected individuals
- Contacts in a childcare centre during outbreaks
- Food handlers working in an establishment with infected individual(s)
- Management
- HAV Ig 0.02 mL/kg IM single dose (within 2 weeks of contact: 80-90% effective)
- HAV vaccine (if unvaccinated, same dosing as for pre-exposure prophylaxis)
Pre-exposure prophylaxis for HBV
| Age (years) | Vaccine | Dose |
|---|---|---|
| < 20 | ENGERIX-B (10 µg/0.5mL) | 3 (0, 1, 6 months) |
| 20 or more | ENGERIX-B (20 µg/1 mL) | 3 (0, 1, 6 months) |
Alternatively,
| Age (years) | Vaccine | Dose |
|---|---|---|
| < 15 | EUVAX B (10 µg/0.5mL) | 3 (0, 1, 6 months) |
| 15 or more | EUVAX B (20 µg/1 mL) | 3 (0, 1, 6 months) |
Post-exposure prophylaxis for HBV
- Indications
- Percutaneous inoculation or transmucosal exposure to HBsAg-positive body fluid (e.g., needle stick injury)
- Direct exposure following sexual contact
- Management
- HBV Ig 0.06 mL/kg IM (ASAP if needlestick, within 14 days if sexual contact)
- Complete HBV vaccination (if unvaccinated, dosing as with pre-exposure)
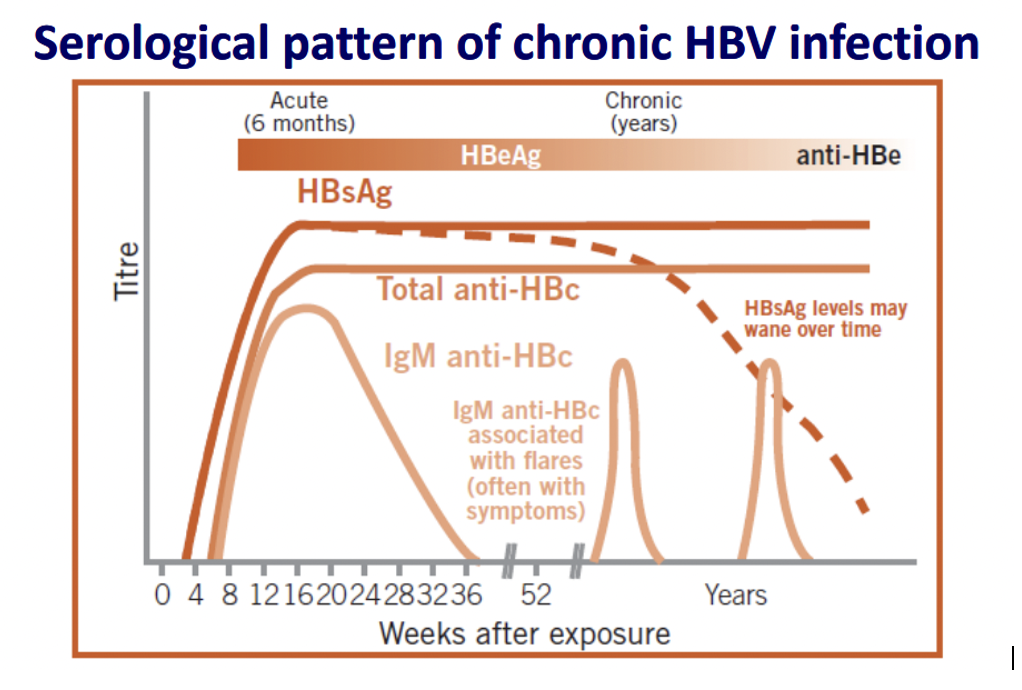
Chronic Hepatitis B
Disease Progression
- Immune tolerance phase: ALT normal, HBeAg +ve, HBV DNA high
- Immune clearance phase: acute hepatitis, abnormal LFT, may lead to hepatic decompensation
- Residual phase: HBe seroconversion (HBeAg -ve but anti-HBe +ve) + liver function may be normal
Investigation
- HBsAg positive > 6 months
| Acute Phase | Serology Profile |
|---|---|
| Early | HBsAg +ve, anti-HBc +ve |
| Window | IgM anti-HBc +ve |
| Recovered (if applicable) | IgG anti-HBc +ve, anti-HBs +ve |
| Chronic Phase | Serology Profile |
|---|---|
| High Infectivity | HBsAg +ve, HBeAg +ve, HBV-DNA high |
| Low Infectivity | HBsAg +ve, HBeAg -ve, anti-HBe +ve, HBV-DNA low |
| Precore mutation individuals | HBsAg +ve, HBeAg -ve, HBC-DNA high |
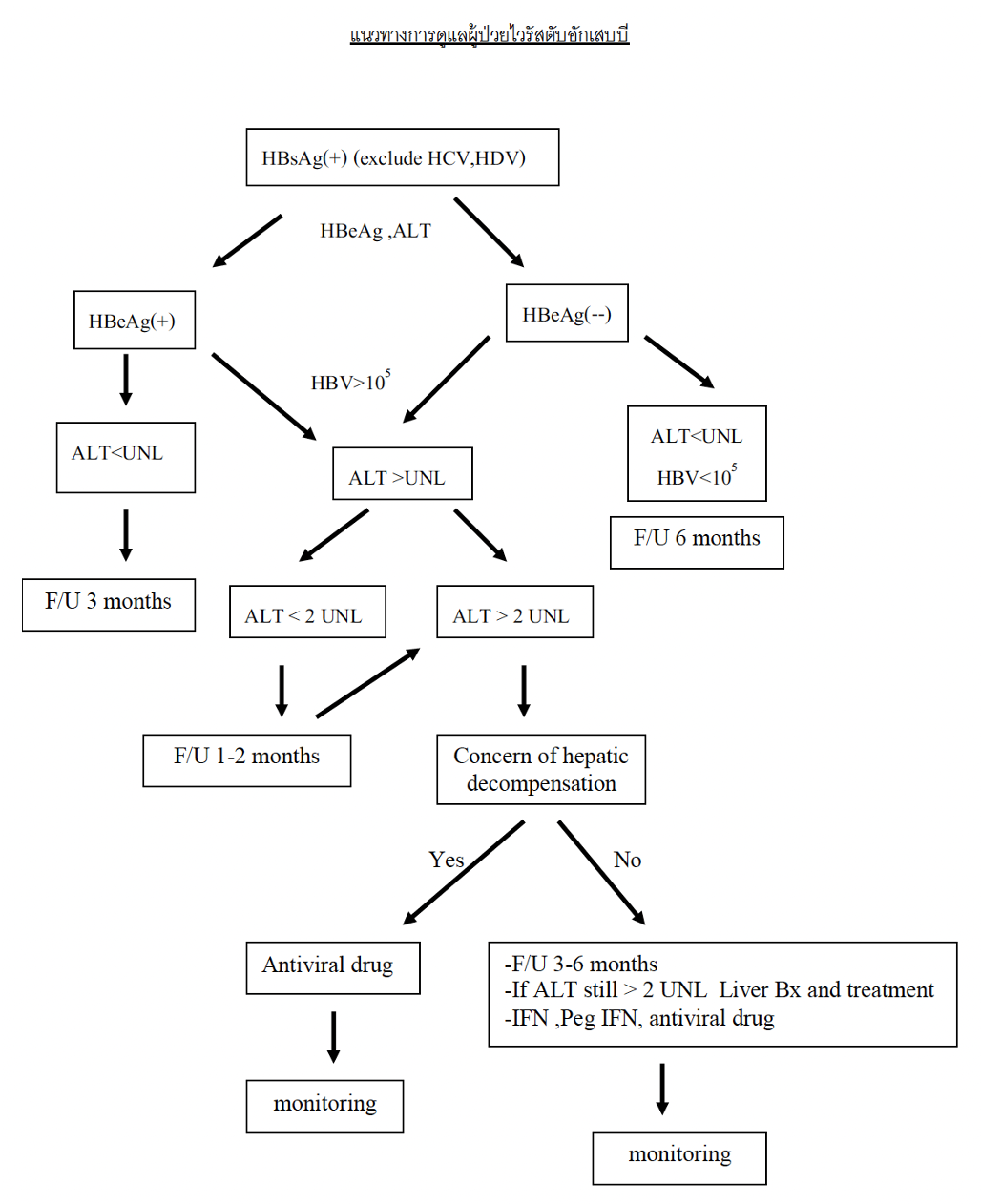
Management
References:
- Survival for all volume 1
- WHO: Training workshop on screening, diagnosis and treatment of hepatitis B