Cardiovascular
Heart Rhythm Disease
Heart Failure
Coronary Artery Disease
Hypertension
Pericardial Disease
Valvular Heart Disease
Vascular Disease
Acute Coronary Syndrome (ACS)
นิยาม
- Acute Myocardial Infarction (MI): positive hs-Tn + (ischemic symptoms หรือ new ST-T change/LBBB หรือ pathological Q wave หรือ positive finding จาก imaging หรือ angiography)
- STEMI: มี ST Elevation (มากกว่า 2.5 ช่องเล็กถ้าเป็น V2-V3 ในชายอายุ < 40 หรือ มากกว่า 2 ช่องเล็กในชาย > 40 หรือมากกว่า 1.5 ช่องเล็กในผู้หญิง หรือ มากกว่า 1 ช่องเล็กใน lead อื่นๆ) หรือ new LBBB
- NSTEMI: ถ้าไม่มี ST Elevation หรือ new LBBB
- Pathophysiology of MI:
- type 1 MI: เกิดจาก intramural thrombus ซึ่งเป็นผลจาก atherosclerotic plaque rupture, ulceration, fissure, erosion, หรือ dissection เป็นต้น
- type 2 MI: เกิดจาก oxygen supply และ demand ไม่สมดุลกัน เช่น coronary spasm, arrhythmias, anemia, hypoxia, หรือ hypotension เป็นต้น
- Unstable angina คือ มี myocardial ischemia แต่ไม่มี myocardial necrosis ซึ่งพบภาวะนี้น้อยลงจากการที่มี high-sensitivity cardiac troponin (hs-Tn) ในกลุ่มนี้จะมีอัตราการเสียชีวิตต่ำกว่า NSTEMI และได้ประโยชน์น้อยกว่าจากการรักษาด้วย intensive antiplatelet therapy หรือ early invasive strategy
Triage
- ผู้ป่วยที่สงสัย ACS (visceral-type chest pain, abnormal vital signs, significant vascular disease risks, dysnea) เข้าสู่ ER
- ประเมินโดยการซักประวัติ ตรวจร่ากายเฉพาะในส่วนที่สำคัญและทำ 12-lead ECG ภายใน 10 นาที (Door to Data) ค้นหาและรักษา life-threatening conditions
ซักประวัติ
- ลักษณะอาการปวด และอาการร่วม: SOCRATES (Site, Onset, Character, Radiation, Associated features, Timing, Exacerbating and relieving factors, Severity)
- Anginal chest pain:
- Central, left-sided crushing chest pain/tightness, radiating to the left jaw and/or arm
- Exacerbated or precipitated by physical activity/exertion
- Relieved or better with rest and/or nitroglycerin
- Types of anginal chest pain
- Typical angina: มีลักษณะครบทั้ง 3 ข้อ
- Atypical angina: มีลักษณะเพียง 2 จาก 3 ข้อ
- Non-anginal chest pain: มีลักษณะเพียง 1 ข้อหรือน้อยว่า
- ประวัติเสี่ยงต่อ ACS เช่น คนสูงอายุ ผู้ชาย เบาหวาน ไขมัน ความดัน ไตเสื่อม ประวัติ CAD, PAD, หรือ carotid artery disease และ ประวัติครอบครัวเป็น CAD
- ภาวะที่กระตุ้นให้เกิด AMI เช่น anemia, infection, inflammation, fever, metabolic, หรือ endocrine (โดยเฉพาะ thyroid) disorders
ตรวจร่างกาย
- ใน NSTE-ACS มักตรวจไม่พบความผิดปกติชัดเจน สิ่งที่อาจตรวจพบ เช่น systolic murmur (ischemic mitral regurgitation), signs of heart failure, electrical instability
- อาจตรวจพบสาเหตุของ chest pain อื่นๆจากการตรวจร่างกาย เช่น
- CVS: aortic dissection, pericarditis, pericardial tamponade, mitral valve prolapse, aortic stenosis
- Resp: pulmonary embolism, pneumothorax, pneumonia, pleurisy
- GI: esophageal rupture (Boerhaave’s syndrome), dyspepsia with reflux, cholecystitis, pancreatitis
- Chest wall pain syndrome: costosternal syndrome, costochondritis (Tietze’s syndrome), precordial catch syndrome, xiphodynia, radicular syndromes, intercostal nerve syndromes, fibromyalgia
- อาจตรวจพบภาวะที่กระตุ้นให้เกิด AMI เช่น anemia, thyrotoxicosis (sweating, tremor)
- การตรวจพบจุดกดเจ็บที่หน้าอกมี NPV ต่อ NSTE-ACS สูง
Investigations
- Laboratory tests: CBC, Cr, glucose, INR ในรายที่ on VKA
- ECG:
- ใน NSTE-ACS พบความผิดปกติจาก 12-lead ECG ได้ประมาณ 2/3 ได้แก่ ST depression, transient ST elevation, T-wave changes
- ถ้า 12-lead ECG ยังไม่สามารถวินิจฉัยได้และยังมีอาการของ ongoing myocardial ischemia ให้พิจารณาทำ V7-V9 (left circumflex) และ V3R, V4R (right ventricle) เพิ่มเติม
- High sensitive-cardiac Troponin
- ภาวะนอกเหนือจาก AMI ที่ทำให้ hs-Tn เพิ่มขึ้น ที่พบบ่อย ได้แก่ tachyarrhythmia, heart failure, hypertensive emergencies, critical illness (เช่น shock, sepsis, burns), myocarditis, Tako-Tsubo cardiomyopathy, structural heart disease (เช่น aortic stenosis), aortic dissection, pulmonary embolism, pulmonary HT, renal dysfunction
- ต้องนึกถึงโรคอื่นที่มาด้วยอาการ chest pain และมี troponin เพิ่มขึ้น เช่น aortic dissection, pulmonary embolism
- Others biomarkers
- เช่น CK-MB มีบทบาทในการวินิจฉัย early reinfraction เพราะ ระดับของ CK-MB ลดลงก่อน cardiac troponin; copeptin ใช้ในที่ที่ไม่มี hs-Tn ในการ early rule-out MI
- Imaging
- CXR แนะนำให้ทำทุกราย เพื่อช่วยวินิจฉัย pneumonia, CHF, esophageal rupture, pneumothorax
- Echocardiography ช่วยวินิจฉัย AMI, aortic dissection, pericardial effusion, aortic valve stenosis, pulmonary embolism
- MDCT ช่วยในการวินิจฉัย CAD (ดู algorithm ด้านล่าง), pulmonary embolism, aortic dissection, tension pneumothorax, esophageal rupture
- อื่นๆ เช่น stress echocardiography, cardiac MRI, nuclear myocardial perfusion, US abdomen
Management
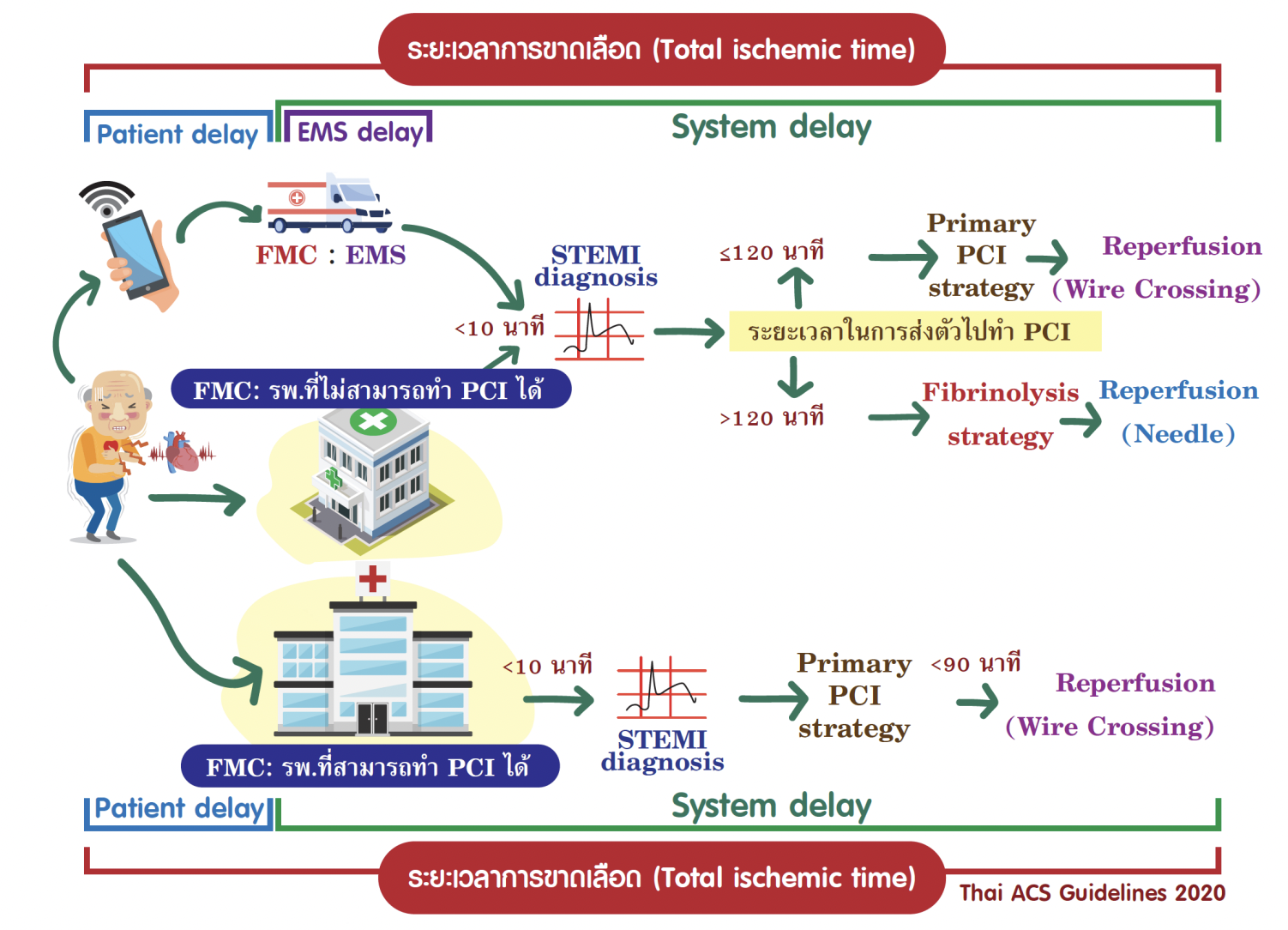
STEMI
- Acute management: MONA (Morphine for pain, Oxygen if SpO2 < 94%, Nitrates, Aspirin (high-dose: 150-300 mg)
- Second antiplatelet เช่น prasugrel, ticagrelor, หรือ clopidogrel
- เป้าหมายคือ reperfusion therapy เช่น PCI ให้เร็วที่สุดถ้าหากว่าสามารถทำได้ภายใน 12 ชม. นับจาก onset ของ chest pain และไม่เกิน 120 นาทีนับจากเวลาที่สามารถให้ fibrinolysis treatment (streptokinase, alteplase, tenecteplase etc.) ได้
- ให้ heparin (unfractionated) ถ้ามี planned PCI ผ่าน radial access หรือ bivalirudin ถ้าผ่าน femoral access
NSTEMI หรือ unstable angina
- Acute management เหมือนกรณี STEMI
- คำนวณ GRACE Score หรือ risk stratification อื่นๆ เพื่อพิจารณาทำ PCI
- ให้ Fondaparinux ถ้าไม่มี plan จะทำ immediate PCI และ bleeding risk ไม่สูงมากนัก (ให้ heparin แทนถ้ามี significant renal impairment)
Secondary prevention (จำไว้เลยครับคนไข้ควรได้ยา 5 ตัวนี้)
- Aspirin ตลอดชีพ
- Second antiplatelet เป็นเวลา 12 เดือนนับจาก ACS
- ACE inhibitor หรือ ARB ตลอดชีพ
- Beta-blocker (ตลอดชีพถ้ามี reduced LVEF ถ้าไม่มี reduced LVEF อาจจะหยุดยาได้หลังจาก 12 เดือน ทั้งนี้ทั้งนั้นต้อง haemodynamically stable นะครับ
- Statin ตลอดชีพ
Reference: ER Goldbook น.พ. รังสฤษฎ์ รังสรรค์