Cardiovascular
Heart Rhythm Disease
Heart Failure
Coronary Artery Disease
Hypertension
Pericardial Disease
Valvular Heart Disease
Vascular Disease
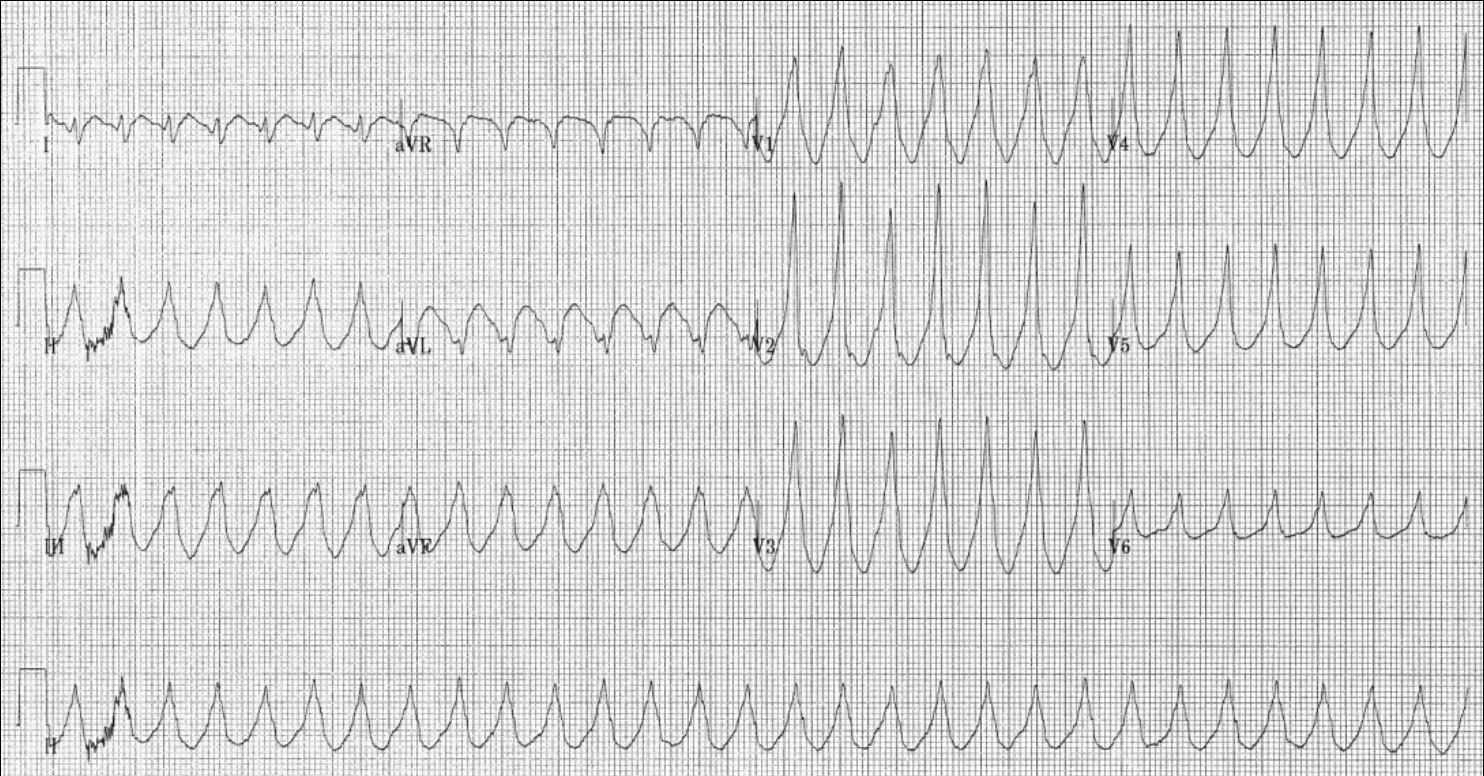
Sustained Ventricular Tachycardia
- Sustained monomorphic ventricular tachycardia (SMVT) is defined as a regular ‘monomorphic’ wide complex tachycardia (QRS > 120 ms, HR > 100) lasting at least 30 seconds
- Often occurs as a consequence of underlying heart disease e.g., MI and other structural heart disease
Signs and Symptoms
- Often lead to haemodynamic compromise: hypotension, chest pain and loss or reduction of consciousness
- Must assess vital signs: pulseless VT is considered a cardiac arrest → initiate advanced cardiac life support (ACLS) immediately
Investigation
- 12-lead ECG or defibrillator pad monitoring
Management
- Haemodynamically unstable patients
- ACLS → starting with a synchronized 120-200 J shock → CPR for 2 minutes and reassess rhythm
- Adrenaline (epinephrine) 1 mg should be given after a second shock (if applicable) and repeat at 3-5 minutes until ROSC or decision to stop resuscitation
- Amiodarone or lidocaine should be given after the third shock if necessary
- Dosing: 1st amiodarone dose = 300 mg, 2nd amiodarone dose = 150 mg; 1st lidocaine dose = 1-1.5 mg/kg, 2nd lidocaine dose = 0.5 – 0.75 mg/kg
- Haemodynamically stable patients
- Trial of pharmacological cardioversion
- Amiodarone, procainamide or lidocaine
- If pharmacological cardioversion unsuccessful → synchronized DC cardioversion 100 J
- Trial of pharmacological cardioversion
- Long-term management consideration: Treat underlying condition, ICD insertion, antiarrhythmic drugs, optimizing heart failure medications, radiofrequency ablation