Cardiovascular
Heart Rhythm Disease
Heart Failure
Coronary Artery Disease
Hypertension
Pericardial Disease
Valvular Heart Disease
Vascular Disease
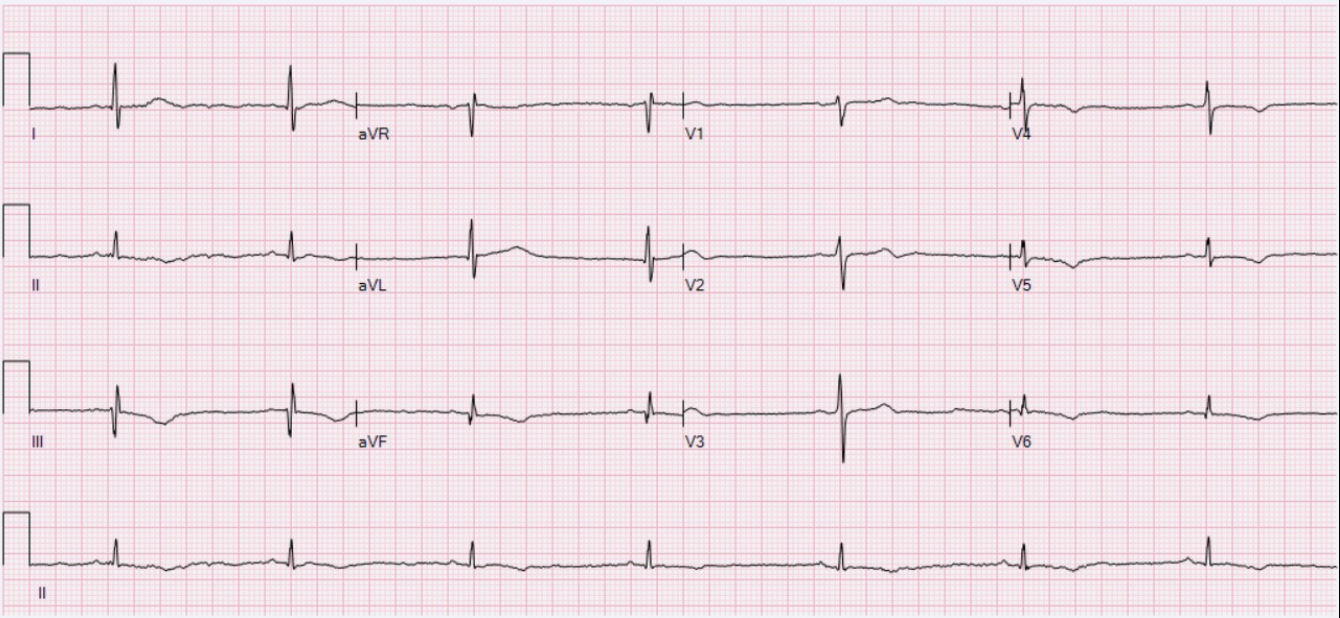
Sinus Bradycardia
- Defined as sinus rhythm with a rate < 60 bpm
- Could be normal in adults or children, particularly when at rest or asleep or athletic.
- Pathophysiologic causes include sinoatrial node disease (e.g., from MI or toxins)
Signs and Symptoms
- Often asymptomatic
- May present as weakness, fatigue, lightheadedness, presyncope or syncope
Investigation
- 12-lead ECG
Management
- If asymptomatic → no treatment required but may consider ETT, TSH and/or Holter monitoring
- If symptomatic
- Haemodynamically unstable → IV atropine 0.5 mg, repeat every 3-5 minutes for a maximum total of 3 mg → transcutaneous pacing if unresponsive to atropine
- Haemodynamically stable → treat underlying cause (MI, toxicity, hypothyroidism) → if not responsive to treatment → permanent pacemaker
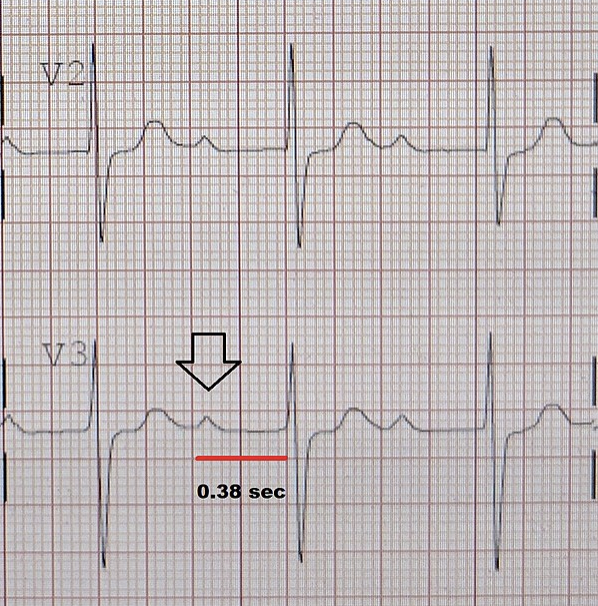
First-Degree AV Block
- PR prolongation > 200 ms with constant PR interval
- Due to delayed or slowed AV conduction
- Can be due to increased vagal tone (physiological) or iatrogenic (e.g. β-blocker, digoxin, rate-limiting calcium channel blocker)
Signs and Symptoms
- Often asymptomatic
Investigation
- 12-lead ECG
Management
- Often not required
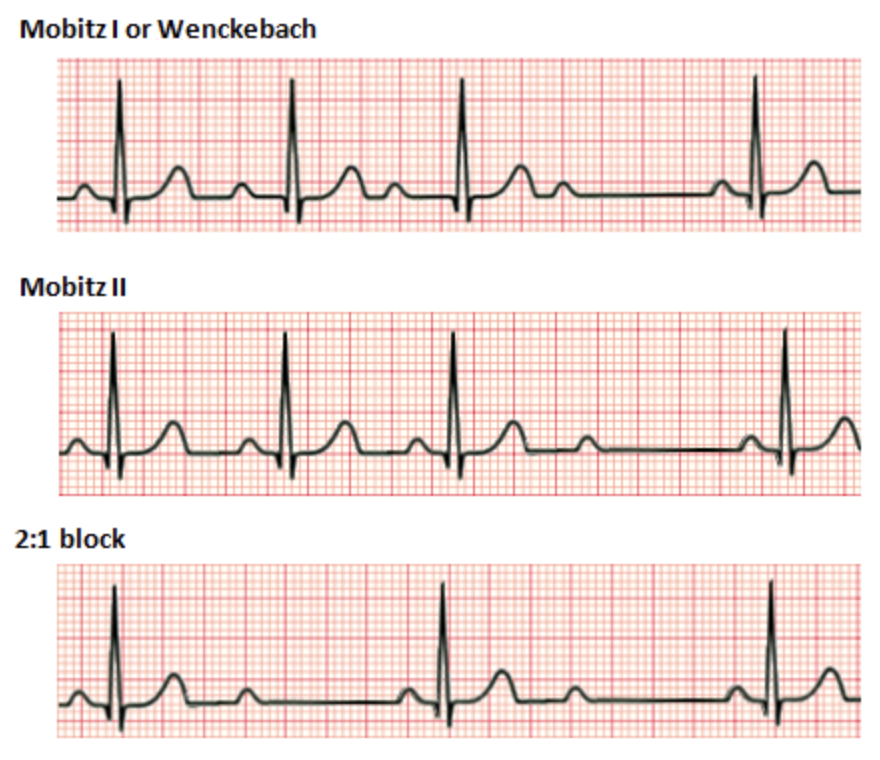
Second-Degree AV Block: Mobitz Type I
- Conduction disorder where some P waves fail to conduct ventricular depolarization
- Progressive PR prolongation
- Also known as Wenckebach block
- Can be idiopathic or secondary to MI, cardiomyopathy, myocarditis, medications or increased vagal tone
Signs and Symptoms
- Often asymptomatic
- When the degree of AV block is high, there may be symptoms associated with reduced cardiac output e.g., dizziness, lightheadedness, presyncope or syncope
- Signs of underlying heart disease: MI, myocarditis, or cardiomyopathy
Investigation
- 12-Lead ECG
Management
- Asymptomatic: no immediate treatment required + treatment of the underlying cause if applicable + ECG monitoring every 6-12 months
- Symptomatic
- Haemodynamically unstable → IV atropine 0.5 mg push (repeat every 3-5 minutes for a maximum total of 3 mg) → if unresponsive to atropine transcutaneous pacing
- Haemodynamically stable → monitoring ECG with transcutaneous pacing pads and prompt treatment if there is deterioration
- Long-term management: treat reversible cause, if none identified then permanent pacemaker (dual chamber DDD)
Second-Degree AV Block: Mobitz Type II
- Conduction disorder where some P waves fail to conduct ventricular depolarization
- Common causes: idiopathic, pathological (MI, myocarditis, cardiomyopathy) or iatrogenic (β-blocker, calcium channel blocker, digoxin, adenosine, antiarrhythmic drugs), increased vagal tone
- The area of AV block is often infranodal
Signs and Symptoms
- Often presents with symptoms of a reduced cardiac output → dizziness, lightheadedness, presyncope or syncope
Investigation
- 12-Lead ECG
Management
- Haemodynamically stable → continuous monitoring with transcutaneous pacing pads in place as Mobitz type II often progresses to a complete heart block
- Haemodynamically unstable → β-adrenegic agonist (dobutamine, dopamine or isoproterenol) → transcutaneous pacing if not responsive to medical treatments
- NB: atropine is often avoided as the Mobitz II block is often infranodal → increasing SA node firing will not improve conduction
- Once patient stable → treat underlying cause if found. If no reversible cause found → dual chamber DDD pacemaker implantation
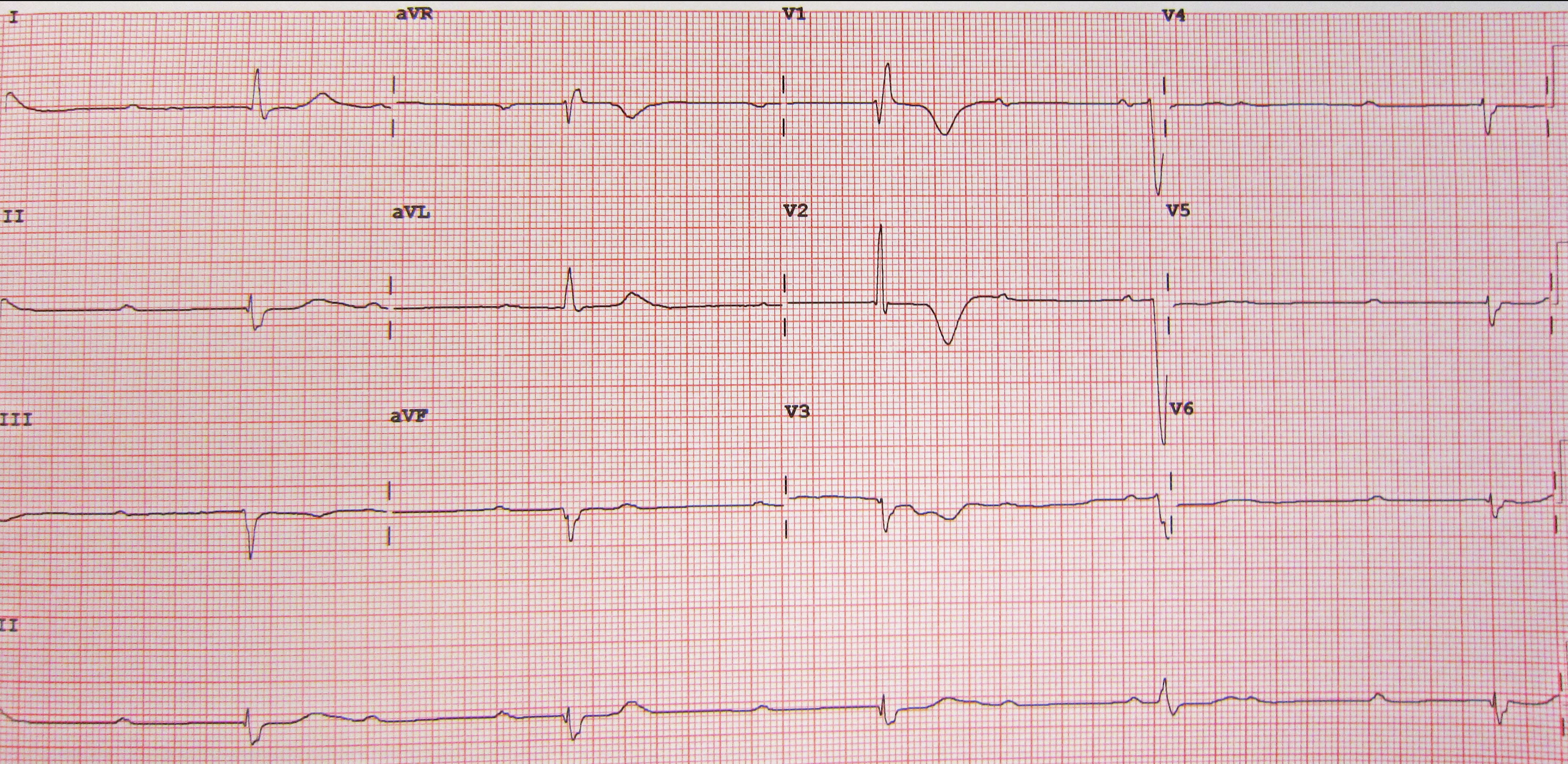
Third Degree or Complete AV Block
- No atrial activities reach the ventricles due to AV nodal or infranodal conduction block
- Common causes similar to second-degree AV blocks e.g. MI, myocarditis, cardiomyopathy or medications
Signs and Symptoms
- Often presents with symptoms of a reduced cardiac output → dizziness, lightheadedness, presyncope or syncope
Investigation
- 12-lead ECG
Management
- Haemodynamically unstable: IV atropine 1 mg STAT + transcutaneous pacing
- Haemodynamically stable: continuous monitoring with transcutaneous pacing pads in place
- Long-term management: treatment of reversible cause → permanent pacemaker implantation if no reversible cause identified
Reference: UpToDate – Atrioventricular Conduction Disease