Cardiovascular
Heart Rhythm Disease
Heart Failure
Coronary Artery Disease
Hypertension
Pericardial Disease
Valvular Heart Disease
Vascular Disease
Acute Heart Failure (AHF)
- Rapid or gradual onset of symptoms and/or signs of heart failure (HF)
- Could be due to new onset HF or acute decompensation of chronic HF (former with higher in-hospital mortality but lower post-discharge mortality)
Clinical presentations
- There are 4 major clinical presentations of AHF
- Acute decompensated heart failure (most common)
- Acute pulmonary oedema
- Isolated right ventricular failure
- Cardiogenic shock
| Acute decompensated heart failure | Acute pulmonary oedema | Isolated right ventricular failure | Cardiogenic shock | |
|---|---|---|---|---|
| Mechanisms | LV dysfunction Sodium and water renal retention | Increased afterload and/or predominant LV diastolic dysfunction Valvular heart disease | RV dysfunction and/or pre-capillary pulmonary hypertension | Severe cardiac dysfunction |
| Main cause of symptoms | Fluid accumulation, increased intraventricular pressure | Fluid redistribution to the lungs and acute respiratory failure | Increased central venous pressure and often systemic hypoperfusion | Systemic hypoperfusion |
| Onset | Gradual (days) | Rapid (hours) | Gradual or rapid | Gradual or rapid |
| Main haemodynamic abnormalities | Increased LVEDP and PCWP Low or normal cardiac output Normal to low SBP | Increased LVEDP and PCWP Normal cardiac output Normal to high SBP | Increased RVEDP Low cardiac output Low SBP | Increased LVEDP and PCWP Low cardiac output Low SBP |
| Main clinical presentations | Wet and warm OR dry and cold | Wet and warm | Dry and cold or wet and cold | Wet and cold |
| Main treatments | Diuretics Inotropic agents/vasopressors Short-term mechanical circulatory support (MCS) or renal replacement therapy (RRT) if needed | Diuretics vasodilators | Same as acute decompensation of CHF | Inotropes or vasopressors Short-term MCS and/or RRT |
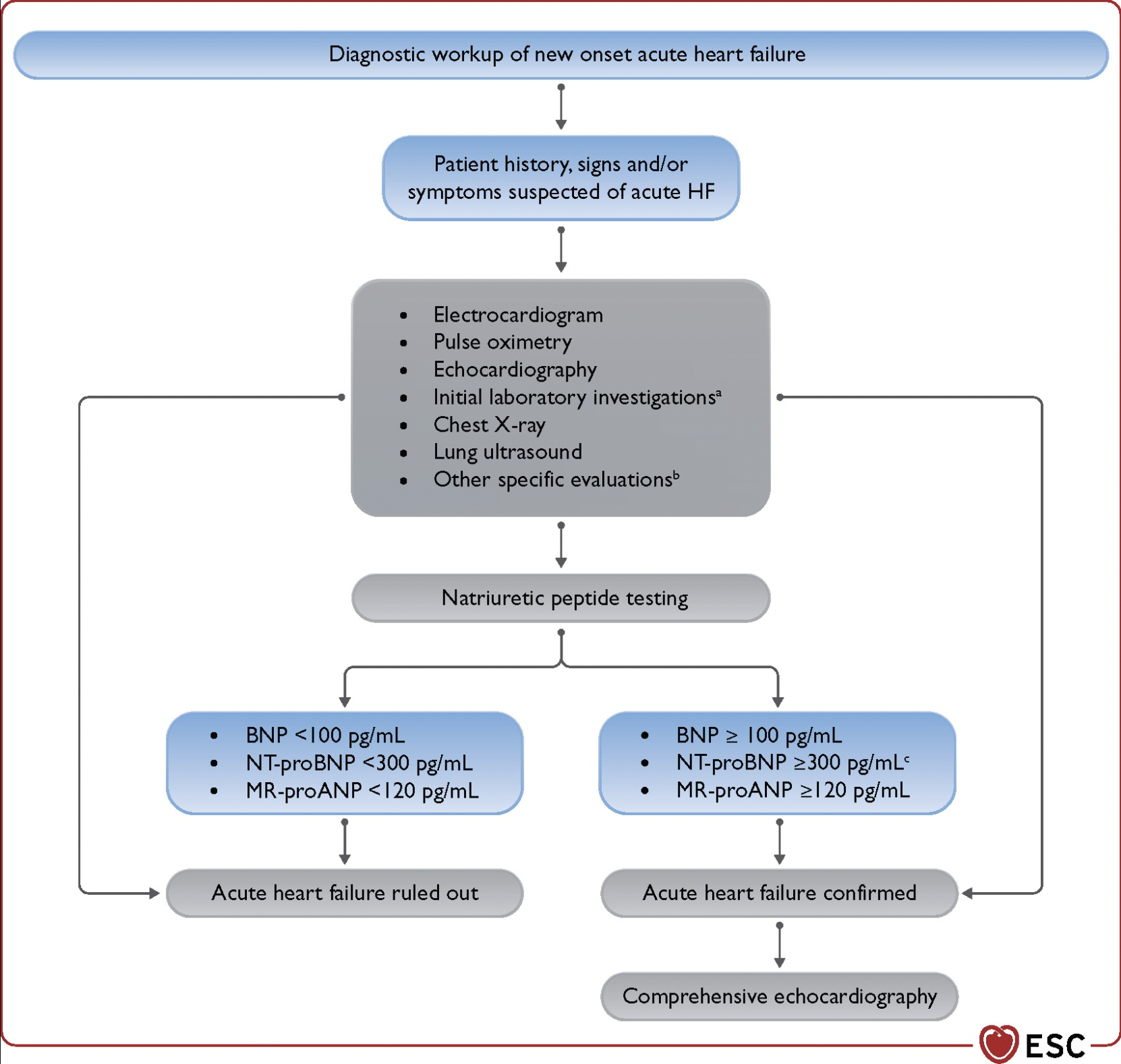
Investigation
- Clinical symptoms in keeping with AHF → test natriuretic peptide level if available
- BNP ≥ 100 pg/mL, NT-proBNP ≥ 300 pg/mL or MR-proANP ≥ 120 pg/mL
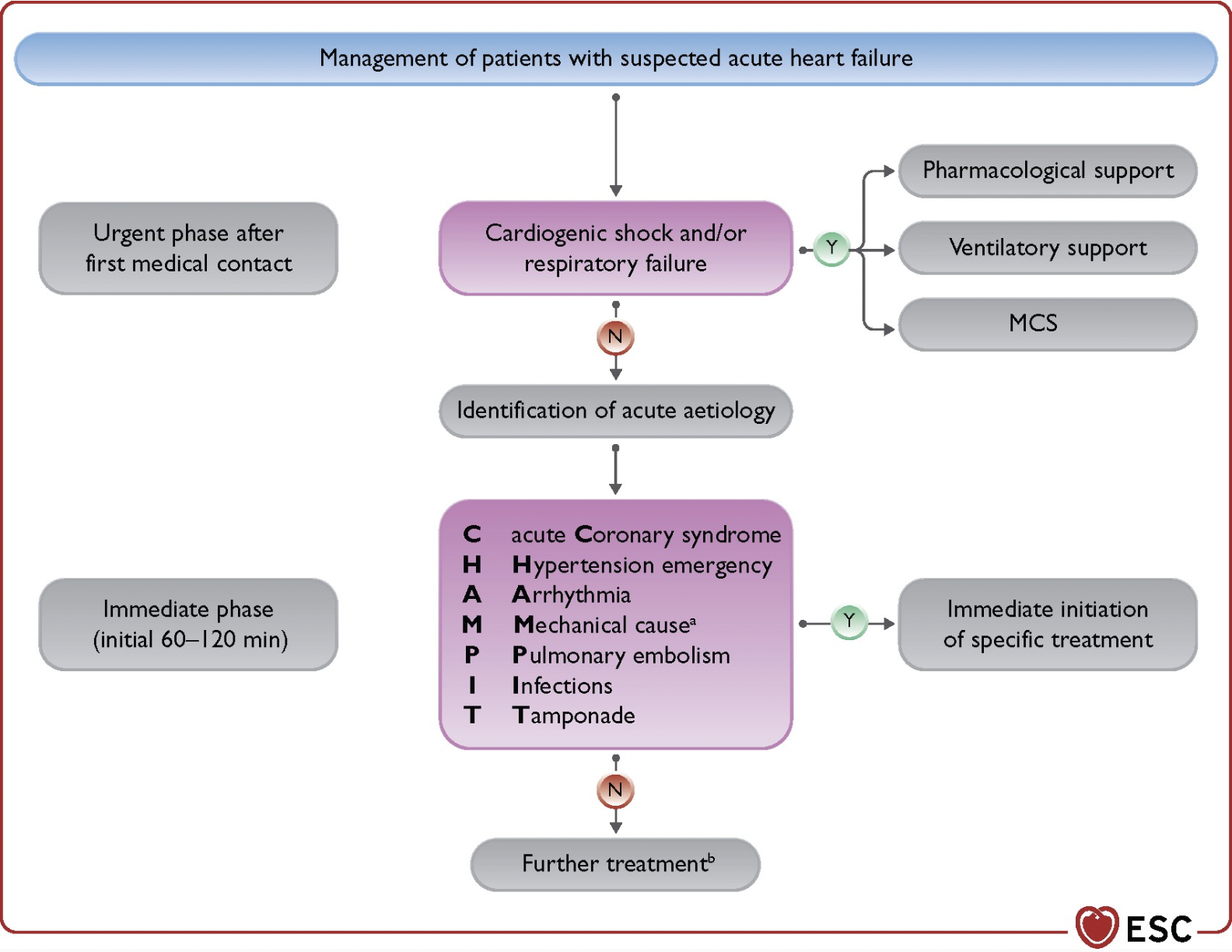
Management
Basic Concepts of AHF Management
- Treatment of congestion = IV diuretics e.g. furosemide
- Treatment of hypoperfusion = inotropes and/or vasopressors
- Treatment of hypoxia = oxygen or ventilatory support
- Last resort managements = MCS and/or RRT
- Acute decompensation
- Treat underlying cause
- Fluid overload/congestion = diuretics
- Hypoperfusion = inotropes and/or vasopressors
- Resistant to medical treatment = consider MCS and/or RRT OR palliative input
- Acute pulmonary oedema
- Treat underlying cause
- Hypoxia = Oxygen supplement or ventilatory support
- Fluid overload = diuretics and/or vasodilator
- Hypoperfusion = inotropes and/or vasopressor
- Resistant to medical treatment = consider MCS and RRT
- Isolated right ventricular failure
- Treat underlying cause
- Fluid overload/congestion = diuretics
- Hypoperfusion = inotropes and/or vasopressors
- Resistant to medical treatment = consider RV assist device and/or RRT OR palliative input
- Cardiogenic shock
- Treat underlying cause
- Hypoxia = Oxygen supplement or ventilatory support
- Hypoperfusion = inotropes and/or vasopressor
- Resistant to medical treatment = consider MCS and RRT
Specific points on management
- Oxygen therapy and/or ventilatory support
- Start when SpO2 90% or PaO2 60 mmHg
- Non-invasive ventilation should be considered if RR > 25 and SpO2 90%
- BP should be monitored during NIV due to possible ↓ venous return and preloads
- Diuretics
- First-line: IV furosemide 20-40 mg (if not on oral furosemide before) or 1-2 times daily oral dose given in 2-3 daily boluses or as a continuous infusion.
- Monitor response → urine sodium > 50-70 mEq/L at 2 hours or urine output > 100-150 mL/h in the first 6 hours
- Decrease dose progressively once negative fluid balance
- Switch to lowest possible oral dose when clinically stable
- Vasodilator
- May be helpful in pulmonary oedema (increased afterload without minimal systemic fluid accumulation) with SBP > 110 mmHg
- Nitrates given as initial bolus followed by continuous infusion
- Up to 1 – 2 mg of nitroglycerine can be given bolus in severely hypertensive patients
- Monitor BP closely (risk of hypotension)
- Inotropes
- Indication = hypoperfusion (low cardiac output, SBP < 90 mmHg or LV systolic dysfunction)
- Side effects: AF, arrhythmias, and MI
- Consider levosimendan or type 3 PDE over dobutamine if patient already on beta-blockers
- Vasopressors
- Used to treat hypoperfusion
- Noradrenaline is preferred in patients with severe hypotension
- Other options: dopamine, adrenaline etc.
- A vasopressor may be used in conjunction with an inotrope if there is cardiogenic shock
- Side effects: increased LV afterload, arrhythmias
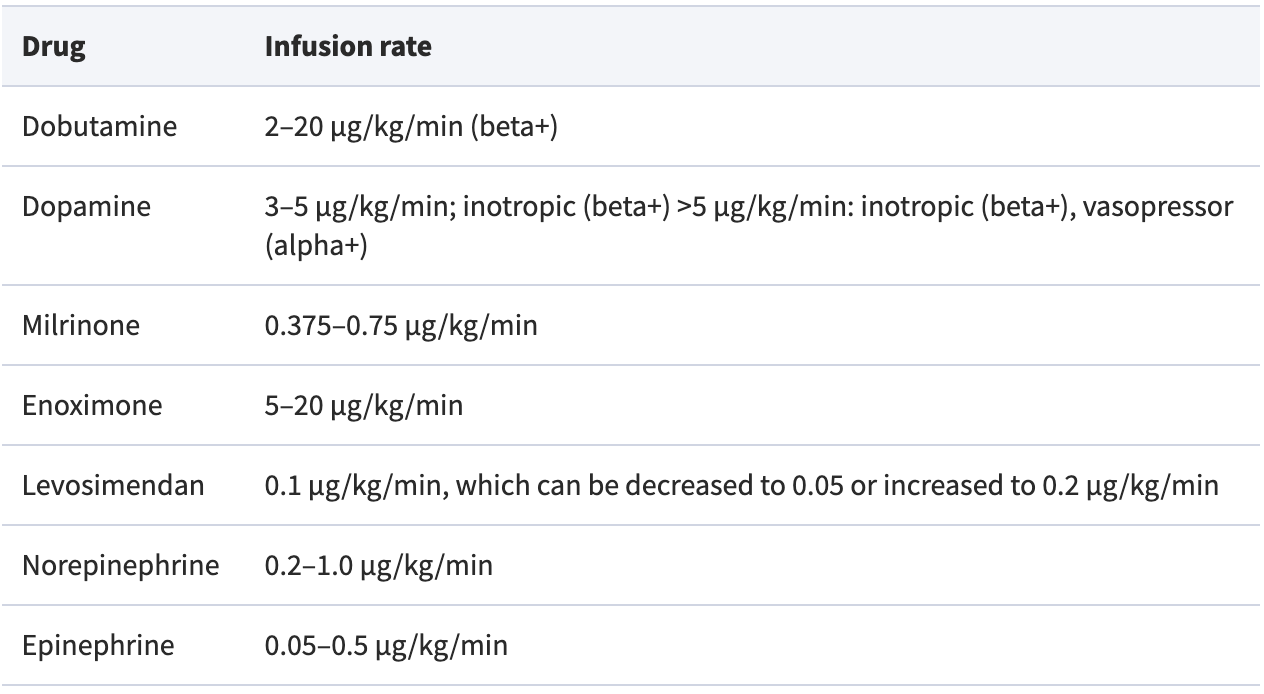
ESC 2021: Inotropes and Vasopressors Dosing for AHF Management
- Routine use of opiates not recommended due to increased frequency of mechanical ventilation, prolonged hospitalization, more intensive care unit admissions and ↑ mortality
- May be considered in severe/intractable pain or anxiety
- Digoxin: may be considered in patients with AHF with fast AF not responsive to beta-blockers
- Mechanical circulatory support → require multidisciplinary expertise. Examples include intra-aortic balloon pump (IABP), extra-corporeal membrane oxygenation (ECMO) and Impella device
Reference: ESC Guidelines 2021